
Published On
January 26, 2023
Author
Oregon Leads the Way for States to Provide Continuous Coverage in Medicaid
Overview
Disruptions in Medicaid coverage, and losing coverage altogether despite remaining eligible, are common occurrences for individuals enrolled in Medicaid. These disruptions and coverage losses result in unmet health care needs, delayed care and increased emergency department use.1 Furthermore, disruptions make it impossible to provide ongoing preventive care and uninterrupted care management for individuals with chronic conditions. The effects are particularly harmful for children given the importance of early interventions, and tend to disproportionately impact people of color and individuals with less education relative to their counterparts.2
Many states agree that continuous eligibility for children is critical. Twenty-four states have implemented the state option to expand continuous eligibility for children enrolled in Medicaid up to 12 months. President Joe Biden recently signed the “Omnibus Bill,” which made that state option a requirement, meaning all states will have to ensure children’s coverage for at least 12 months. Oregon has taken this one encouraging step forward with a September 2022 approval of their 1115 demonstration, becoming the first state authorized to provide multiyear continuous Medicaid enrollment for children and adults to minimize coverage disruptions. Oregon’s policy covers children from the time of initial Medicaid or Children’s Health Insurance Program (CHIP) eligibility determination until they reach age 6, and provides two years of continuous enrollment for adults and children ages 6 and older.3, 4
The article below describes the context and approach that led to this policy approval and is a helpful roadmap for other states considering this Medicaid coverage expansion.
Coverage Disruptions and the Value of Continuous Enrollment
There are a variety of reasons for disruptions in Medicaid coverage, often referred to as “churn.” It may be that an individual experiences an income fluctuation due to overtime pay or a temporary second job that briefly makes them ineligible. Income fluctuations are more frequent among people with lower incomes, people of color and individuals with less education.5 Churn often occurs due to administrative reasons, such as difficulty navigating the renewal process, including securing required documentation or failing to receive the renewal request due to a change in address.
These Medicaid coverage disruptions result in a 10 to 36 percent increase in emergency department use, office visits and hospitalizations, and dampen the use of prescription medications by 19 percent, compared to individuals with consistent Medicaid coverage.6
For children, early detection of and timely intervention for developmental delays, including screenings conducted during early childhood well visits, have been shown to positively impact health, language, communication and cognitive development.7 Considerable evidence indicates that a strong foundation of coverage and continuity of care can help children be school-ready, ensure timely referrals to Early Intervention services, and potentially lower special education and child welfare costs.8
Continuous enrollment also makes expenditures more predictable, reduces administrative costs and, potentially over time, lowers monthly member costs. Studies show the average monthly cost for a child enrolled in Medicaid for 12 months was $107, compared to $163 for a child enrolled for only one month and $147 for a child enrolled for only six months.9
Building and Sustaining Support for Continuous Enrollment in Oregon
Oregon’s continuous enrollment policy was motivated by state efforts to focus attention on the needs of kids and families. In 2017, former Governor Kate Brown convened a Children’s Cabinet of leaders across multiple state disciplines to develop programs and pathways focused on supporting children and families living in poverty. This work served as a springboard for state agencies, including the Oregon Health Policy Board (OHPB), to begin exploring ways in which the state could incentivize the Coordinated Care Organizations—Oregon’s managed care organizations—to prioritize care and coverage for young children.
In 2019 the Oregon Health Authority (OHA), in partnership with the Oregon Pediatric Improvement Partnership (OPIP), received $16 million in funding from the Centers for Medicare & Medicaid Services’ (CMS) Integrated Care for Kids Model to improve health for children and youth covered by Medicaid and CHIP. OHA and OPIP’s work on the model highlighted the experience of families with complex health and social circumstances and the barriers to consistent coverage, laying a strong foundation to make continuous coverage, particularly for children, a central component of Oregon’s upcoming 1115 demonstration renewal.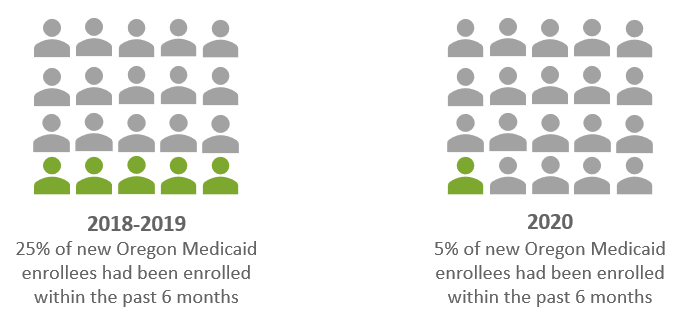
To gain a deep understanding of the extent of churn in Oregon’s Medicaid program, Oregon compared its enrollment data before the COVID-19 Public Health Emergency (PHE) with enrollment during the PHE to understand how the continuous Medicaid coverage provision of the PHE had impacted its Medicaid enrollment and retention. Oregon found that from 2018 to 2019, 25 percent of new Medicaid enrollees had been enrolled within the past six months, implying a significant amount of churn. During the last six months of 2020, this number dropped to just 5 percent. This indicated that despite Oregon’s relatively high insurance rates, churn had been a real issue that was largely addressed by the continuous enrollment provision. Notably, data from the PHE showed the gap in coverage rates between Black and white Oregonians shrunk from about 2.8 percentage points in 2019 to less than 1.6 percentage points in 2021.
Buoyed by agency and state support, Oregon began drafting concept papers for its demonstration renewal in 2021 and released drafts for comment in November 2021. The public input and engagement, both on the concept papers and the draft waiver application, helped clarify the problems that families were facing and refine the policy proposal for continuous coverage. OHA received overwhelmingly positive feedback for the continuous enrollment proposal.
Ultimately, Oregon crafted a vision for its 1115 demonstration—to advance health equity through a four-pronged approach, one of which being to ensure people maintain their health coverage. Specifically, throughout the five-year waiver demonstration, Oregon sought to reduce its current uninsured rate of 4.6 percent to less than 2 percent, while also eliminating racial and ethnic disparities in the uninsured rate.
CMS Negotiations and Approval
In partnership with CMS, OHA further refined the policy, including who would be eligible, how the state would conduct eligibility redeterminations at the end of the continuous eligibility period, and the federal match rate available to the state. Under the final demonstration approved by CMS in September 2022:
- Eligibility: All CHIP and Medicaid eligibility groups, except for individuals eligible for Medicaid solely on the basis of qualifying for home and community-based services, are eligible under the policy.
- Redetermination: CMS requires that the state conduct full redeterminations at the end of the individual’s continuous enrollment period. Though not a requirement, the state will continue to do “shadow” annual redeterminations as they have been doing throughout the PHE, which allow the state to move people between eligibility categories (i.e., from CHIP to Medicaid). No one will lose eligibility as a result of these shadow redeterminations, even if they are found to be over-income. During the continuous enrollment period, an individual will only experience a redetermination or a termination of coverage if they move out of state, if they request termination, if eligibility was granted due to agency error, or in the event of death.
- Budget Neutrality: For all 1115 demonstrations, the federal government requires that they be budget neutral, meaning they do not cost the federal government any more than they would have cost without the demonstration. For this policy, all of the costs will be treated as hypothetical for the purposes of budget neutrality. CMS determined the continuous coverage provision largely protects individuals who are already eligible from losing coverage, and as such, any associated costs will be excluded from the budget neutrality calculation.
- Federal Medical Assistance Percentage: Match rate is generally not implicated by demonstration approvals except with respect to the enhanced match rate for adults in the ACA expansion group. CMS has generally estimated that 2.6 percent of the adults in that group will experience a change in income that would put them over the eligibility level for that group, which is matched at an enhanced rate. To adjust for this, CMS will apply the regular Federal Medical Assistance Percentages (FMAP) (rather than the enhanced FMAP) for 2.6 percent of the individuals enrolled in the Medicaid New Adult Eligibility Group. This does not impact the match rate for any other group, including children.
Conclusion
Continuous enrollment for Medicaid beneficiaries will lead to improved health outcomes, more predictable costs and more consistent preventive care. Given that 12-month continuous coverage for children is now mandatory, and the broad enthusiasm from children’s health care providers and advocates and support from CMS for broader, multiyear expansion beyond 12 months, other states are likely to seek to build on Oregon’s approach and pursue similar 1115 demonstrations.
1 Banerjee, R., Ziegenfuss, J. Y., and Shah, N. D. Impact of discontinuity in health insurance on resource utilization. BMC Health Services Research, 10(1), 1-10. July 2010. Available here.
2 Association for Community Affiliated Plans. FAQs: Churning, Continuous Eligibility and Administrative Burden. Available here.
3 Washington has a similar 1115 demonstration request pending; it has requested to provide continuous coverage to children with incomes up to 215 percent of the federal poverty level (FPL) up to age six. New Mexico also has an 1115 demonstration renewal request under review with CMS and similarly includes continuous enrollment for children up to age six. A 2022 California state law requires that the state implement continuous enrollment for children up to age five no sooner than January 2025, contingent on federal approval and state appropriations.
4 Most individuals will be covered by the policy except for individuals who are eligible for Medicaid on the basis of eligibility for home and community-based services under 42 CFR § 435.217 (available here).
5 Sugar, S., Peters, C., DeLew, N., and Sommers, B.D. Medicaid Churning and Continuity of Care: Evidence and Policy Considerations Before and After the COVID-19 Pandemic (Issue Brief No. HP-2021-10). Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. April 2021. Available here.
6 Banerjee, R., Ziegenfuss, J. Y., and Shah, N. D. Impact of discontinuity in health insurance on resource utilization. BMC Health Services Research, 10(1), 1-10. July 2010. Available here.
7 Center on the Developing Child at Harvard University. The Foundations of Lifelong Health Are Built in Early Childhood. July 2010. Available here.; Guralnick, M.J. and Bricker, D. The Effectiveness of Early Intervention for Children with Cognitive and General Developmental Delays. In: The Effectiveness of Early Intervention for At-Risk and Handicapped Children. San Diego, CA: Academic Press; 1987:115-173. Available here.; Hebbeler, K., Spiker, D., Bailey, D., et al. Early intervention for infants and toddlers with disabilities and their families: participants, services, and outcomes. January 2007. Available here.
8 Currie, J. Early Childhood Intervention Programs: What Do We Know?. April 2000. Available here.
9 Whitener, K. and Snider, M. Advancing Health Equity for Children and Adults with a Critical Tool: Medicaid and Children’s Health Insurance Program Continuous Coverage. Georgetown University Health Policy Institute Center for Children and Families and UnidosUS. October 2021. Available here.