
Published On
May 28, 2026
Authors
Optimizing Regional Cancer Service Lines: Challenges and Strategies
Introduction
While the U.S. is home to many of the world’s leading cancer centers, the majority of care—approximately 85%—is delivered in community settings. In response, community hospitals have continued to invest in strengthening their oncology capabilities, and Academic Medical Centers (AMCs) have expanded into broader Academic Health Systems (AHSs) through the acquisition of, or affiliation with, community hospitals. These systems are focused on extending high-quality cancer care closer to patients’ homes while enhancing access for complex cases who need the AMC-level of advanced care. The goals for regional cancer service lines are to: provide access to the same level of state-of-the-art care for all patients, grow volume overall, and optimize financial performance.
It is, however, not an easy task to organize the delivery of cancer care across a regional system. An AHSs’ ability to do this well is also influenced by the maturity and effectiveness of their system operating model with many still evolving., As AHSs work to implement regional cancer service lines, we describe the challenges and offer strategies to consider.
Regional Health Systems and Cancer Service Lines
Cancer programs in a single hospital are more complex than other service lines because they depend on multiple specialties and services. This complexity is amplified when care is delivered across multiple hospitals within a region and further complicated when it involves an AMC and community hospitals due to their different structures, cultures and level of system integration. While systems seek to leverage the AMC’s clinical reputation to attract and retain patients, many efforts fall short because they underestimate the level of coordination required and related difficulty in execution. Successful regional cancer service lines require sustained executive leadership, clear strategic direction and strong engagement from physicians and administrators across the system.
Challenges
- Clinical practice variation—Planning may not fully address how to deploy disease site specialists, including surgeons, and medical oncology generalists effectively. Complexities include managing clinical, academic and research goals, different clinical workload and compensation structures across the AHS, and the need for mechanisms to facilitate coordination and communication to leverage expertise. In many cases, community-based cancer specialists are not employed, which can make alignment more difficult.
- Conflicting financial goals within the system—Individual entities in an AHS often seek to optimize margins from cancer care within their siloes, which can create misalignment and make it harder to balance both bringing advanced care to the community and referring patients to the AMC when appropriate. Entities include the hospitals but also the academic departments and divisions, the faculty practice plan and other physician organizations that may be part of the system—each with financial performance targets as most often there is not an integrated service line budget.
- Insufficient decision rights for service line leadership—Regional cancer service lines in an AHS are highly matrixed and program management may have limited authority to make decisions to advance the system service line.
- Program variation across the system—State-of-the-art cancer care requires comprehensive high quality clinical and patient support services, including access to clinical trials. There is often variation across a system with locations having varying levels of quality and access, as well as different capacities to invest in or provide services (i.e., patient navigation, genetics, palliative care, psychosocial care), and limited standardized data and reporting to support the needed analyses.
- Disruption of local market dynamics and referral patterns—Cancer referral patterns from surgeons and primary care physicians are local. They can be disrupted and impact revenue if managing these relationships for each location is not factored into regional service line strategies.
Key Enablers of an Effective AHS Distributed Regional Cancer Service Line
System-level senior leadership of the AHS must establish the vision and drive the planning and investment to overcome challenges and achieve the goals with key enablers described below.
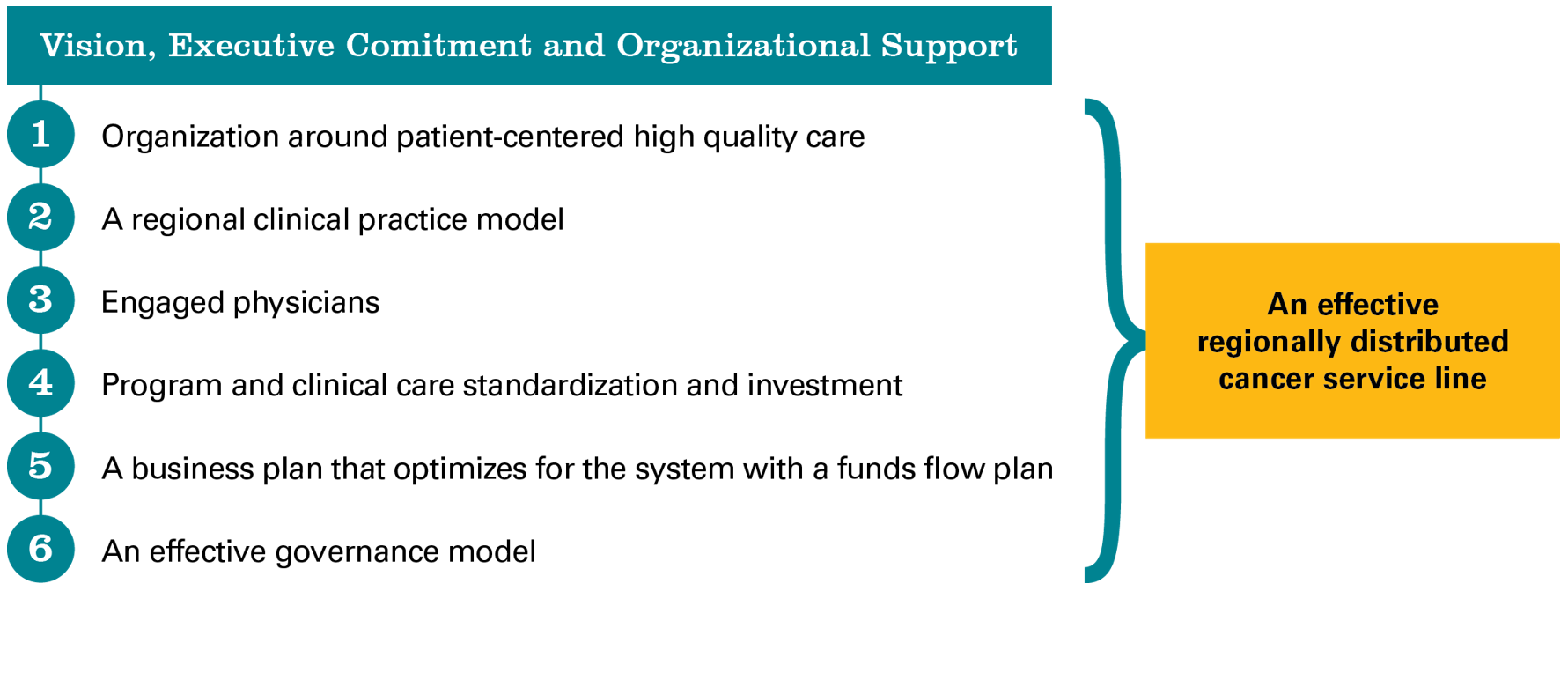
- Organization around patient-centered high-quality care—The success of a regional cancer service line depends on systemwide support for a common goal of organizing around the patient and quality care including access to clinical trials as close to home as possible. The benefit of this model is to have volume and revenue growth overall, even if volume shifts from the AMC. Ideally shifting volume will improve access at the AMC. System leadership will have to establish this goal and ensure that barriers are addressed during planning and implementation.
- A regional clinical practice model—A clinical practice model for the continuum from the AMC to the community hospitals across cancer specialties will need to consider: how best to standardize care, when to refer a patient to a specialist at the AMC, when AMC disease site specialists and surgeons should have sessions at the community hospitals, or community sites, if/when surgeons should perform procedures in the community, when patients can be referred for ancillary services close to home, what support or specialized technology is needed in the community and how to support clinical trials in the community. The financial and operational implications and requirements of the model have to be assessed and addressed in planning.
- Engaged physicians—Buy-in from the AMC and community-based physicians is critical across specialties, frequently requiring outreach, representation and financial considerations. In many cases, AMC disease site specialists and surgeons will have clinic sessions in the community, which will require practicing at more than one location, which may not be embraced. Local physicians who are not employed or with Professional Services Agreement (PSA) arrangements will have to be included in planning and have their requirements met. It is important to facilitate strong AMC/community cancer specialty physician relationships and for local referral relationships to be preserved and expanded.
- Program and Clinical Care Standardization and Investment—The same level of quality and program components should be available at each location, which requires an assessment, a plan to achieve and investment. This includes mechanisms to standardize care (i.e., care pathways), the same level of Lab/Pathology and Diagnostic Imaging expertise and service, similar program components (i.e., patient navigation, psychosocial care, palliative care, genetics, access to clinical trials) and systems to support such as data analytics and the same EMR, which is not always possible in the short term.
- A business plan optimizing for the system with a funds flow plan—The financial implications of the care delivery model and how to optimize for the system must be assessed and planned for with funds flow adjustments as needed. For example, a surgical specialist scheduled for clinic sessions and/or procedures in the community may reduce cases and margin at the AMC or for the faculty practice plan, but be beneficial overall for attracting new local patients to the system. The plan must include revenue and expense modeling and a Return on Investment analysis overall and at the entity level. An effective governance model—Dyad leadership of a physician and administrator is essential for the management of a distributed regional cancer service line with reporting at a high level within the system. The system service line will have to align with local level service line or program structures. A multi-level governance model is needed to enable strategic direction and accountability, effective operations and key stakeholder engagement. Each group must have a clear charter and a focus on goal achievement. Representatives from each location need to be included
- An effective governance model—Dyad leadership of a physician and administrator is essential for the management of a distributed regional cancer service line with reporting at a high level within the system. The system service line will have to align with local level service line or program structures. A multi-level governance model is needed to enable strategic direction and accountability, effective operations and key stakeholder engagement. Each group must have a clear charter and a focus on goal achievement. Representatives from each location need to be included.
To inform the vision and plans, baseline data and information should be collected as outlined in Box 1 and used to set performance targets that are monitored.
Conclusion
Successfully optimizing a distributed regional cancer service line in an Academic Health System requires more than extending the AMC brand into the community; it demands deliberate system design that aligns clinical practice, program capabilities and economics across multiple entities. As highlighted, variation in clinical practice, competing financial incentives, limited decision rights, uneven program infrastructure and disruption of established referral patterns can quickly undermine the goals of improving access to high-quality care close to home while appropriately channeling complex cases to the AMC.
Addressing these barriers starts with clear system-level vision and sustained executive sponsorship, informed by baseline data on outmigration, finances, specialist resources, program gaps and referral sources. With an agreed-upon regional clinical practice model, engaged physicians, standardized program components (including pathways, diagnostics, supportive services and clinical trials access), an enterprise business plan with workable funds flow, and governance with accountability, AHSs can deliver consistent, state-of-the-art oncology care across the region. Done well, this model provides access to the same level of quality care and patient experience, strengthens market position and supports growth, and optimizes financial performance for the system as a whole.
Box 1: Preliminary Data to Collect by Major Disease Site for Planning/Strengthening an AHS Distributed Regional Cancer Service Line
|
O’Brien D, Pawlak B, Ingraham M, Academic Health System Cancer Programs: Eight Fundamental Elements to Reassess in the New Environment, Manatt Health. September 2025.
Enders T, Maintaining the Integrity of the Missions: Academic Medicine Participation in Health Care Consolidations, Manatt White Paper, July 2025.
Enders T, Brown D, Robertson T, Governance Renewal for Health Care Systems: Managing the Transition to Operating Company Models. Manatt White Paper, May 2026.
Fracasso PM, Simone NL, Si Lim SJ, Reckamp KL, Sosa JA, Lieu C, Lee C, Werner TL, Ly QP, Vose JM, White J, Honeycutt H, Shaw K, Cameron K, O'Brien DM, Wilke LG. Benchmarking the Current Landscape: Insights From an Association of American Cancer Institutes Survey on Academic Cancer Service Lines. JCO Oncol Pract. 2025 Sep 24:OP2500073. doi: 10.1200/OP-25-00073. Epub ahead of print. PMID: 40991878.