
Maternal Health Innovations Through the Rural Health Transformation Program
Through the federal (RHTP), many states are prioritizing maternal and infant health using RHTP funding to address workforce shortages and access barriers, expand telehealth-enabled prenatal and postpartum care, and invest in community resources and supports for pregnant and postpartum Medicaid members, their newborns, and families.
With a deadline of October 30, 2026 to obligate first-year awards, states are accelerating design, implementation and funding decisions for their RHTP plans, many of which include initiatives focused on improving maternal and infant health outcomes in rural communities.
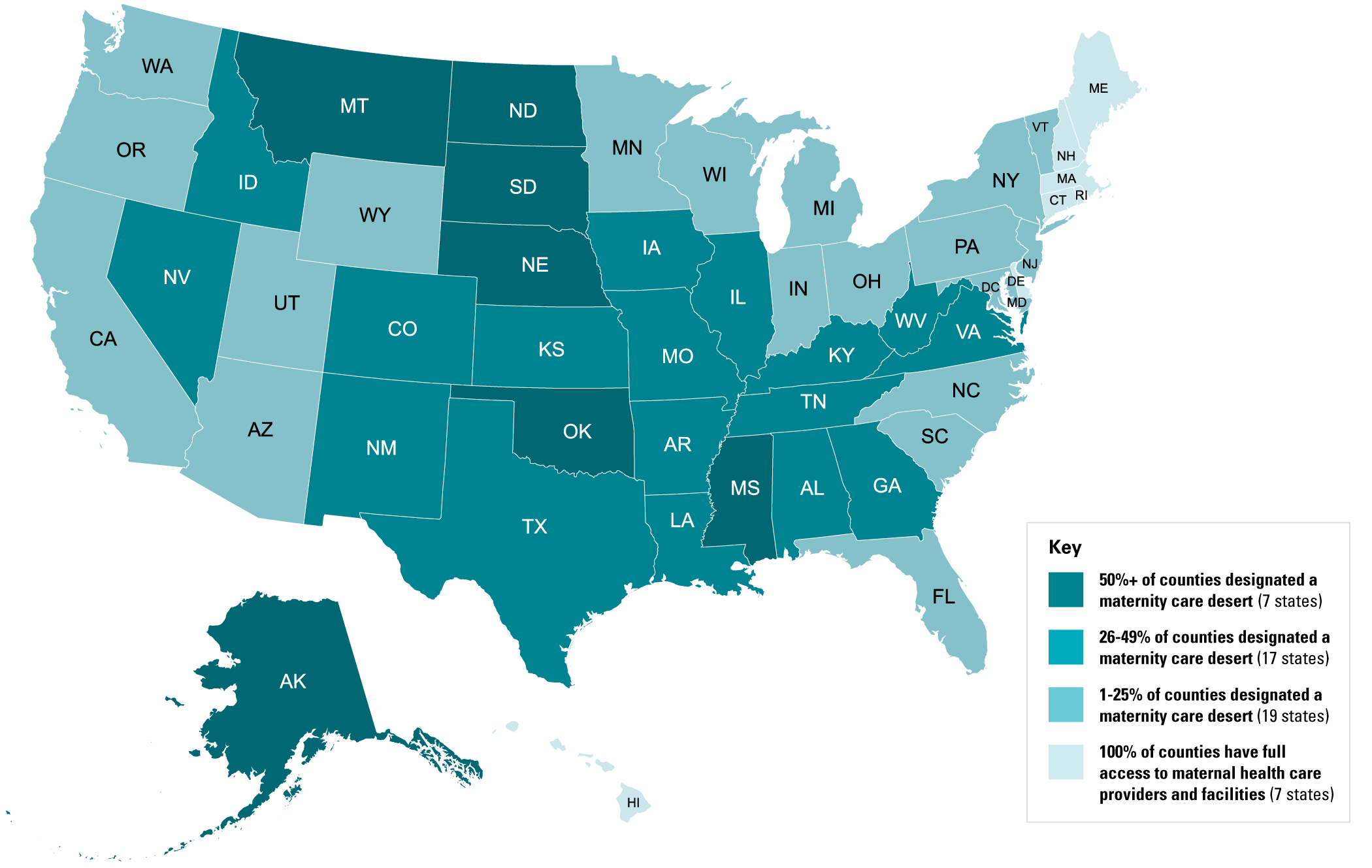
Figure 1: Maternity Care Deserts in the United States
Many states are trying to address these myriad challenges through the RHTP. An analysis of states’ RHTP applications identified key areas that states are seeking to address to improve maternal health in rural communities.
Mitigating Maternity Deserts
One in three counties nationwide is considered —lacking a hospital, birth center or obstetric provider—which can put pregnant and postpartum people and their newborns at risk during prenatal, labor and delivery, and postpartum periods (see Figure 1). Over 130 rural labor and delivery units have since 2020. States are aiming to address the disparity in access to obstetric care in rural counties by proposing financial and operational pathways to sustain low-volume labor and delivery units and reopen closed facilities for low-risk births.
- Alabama expanding an existing pilot program that deploys emergency labor and delivery carts to rural hospitals and uses telerobotic ultrasound machines to address OB/GYN shortages and hospital closures.
- Alaska converting underused patient rooms into family-friendly maternity spaces.
- New Mexico to develop an incentive payment model for rural hospitals and clinics that establish and sustain maternal and specialty care service lines for high-need, high-cost populations.
Workforce Expansion and Upskilling
The federal government an OB/GYN shortage of 46% in nonmetro areas in the next ten years. To address OB/GYN shortages, states are considering investments in other maternal health care providers. In recent years, state Medicaid programs have expanded access to doulas, CHWs, and midwives with all states reimbursing (CNMs) and more than two dozen states reimbursing for Medicaid coverage of and care. However, , and have reported challenges accessing Medicaid reimbursement, working with broader obstetric care teams and hospital systems, securing licensure and operating under their full scope of practice.
- California to support the development of nonphysician maternal health care roles to strengthen access to quality, community-based maternal health care services, primarily with CHWs, doulas, midwives and local vocational nurses.
- Iowa the High-Risk OB & Neonatal Transport Project to transport high-risk maternal and infant cases from rural hospitals to specialized care settings, supported by specialized obstetric training for the EMS workforce to operate at the top of their license and ensure quality care during transport.
- Missouri to create an in-state training program for CNMs with an accredited nursing school.
- Nebraska is a statewide Maternal-Fetal Medicine Rural Provider Pairing Program to connect primary care rural providers in rural areas with obstetricians, with providers co-managing high-risk pregnancies through telehealth capabilities.
- New York advanced training in pregnancy support, lactation counseling and simulation-based obstetrics for a range of providers in rural counties and maternity care deserts, including EMTs, nursing students and medical students.
Digital Hub-and-Spoke Regionalization
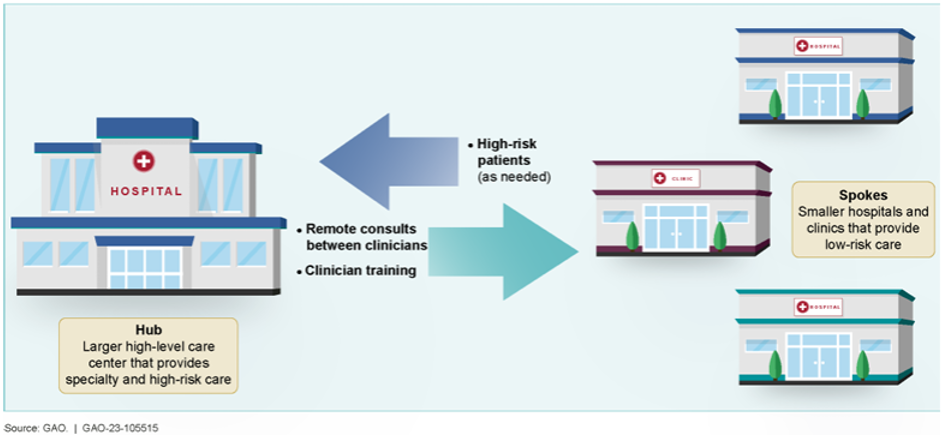
From 2021 to 2022, one in every 25 obstetric units has nationally. In response, many states’ RHTP applications propose regional maternal health hubs that connect rural clinics (“spokes”) to academic medical centers and maternal-fetal medicine specialists (“hubs”). This hub-and-spoke model uses telehealth, remote patient monitoring for gestational diabetes and hypertension, and telerobotic ultrasounds to keep high-risk pregnant people safely in their communities.
Figure 2: Illustration of Hub-and-Spoke Model
- Kentucky a telehealth-enabled care team of perinatal CHWs, doulas and peer support specialists operating in maternity care deserts, partnered with a local health department, rural health clinic, or federally qualified health center.
- Oklahoma also remote patient monitoring with blood pressure cuffs for pregnant individuals with hypertension. The state also aims to ensure high-risk pregnant individuals have access to maternal-fetal medicine providers via telehealth expansion.
- Pennsylvania to deploy remote patient monitoring to manage high-risk pregnancies and postpartum complications in 48 of the state’s 69 , including prompt interventions with tele-maternal-fetal medicine consults when needed.
- South Dakota to support the design and launch of “OB-Nest”-style programs at three health care entities. First developed by the Mayo Clinic, the OB-Nest model is a virtual prenatal and postpartum care program that allows patients to travel less with virtual visits and at-home remote patient monitoring.
Evidence-Based Safety Bundles and Quality Collaboratives
States are proposing to use RHTP funds to mandate and support evidence-based standardization of facilities’ responses to maternal health care emergencies, such as obstetric hemorrhage and preeclampsia, to ensure pregnant people giving birth across a state have the same facility experience whether they are in a rural or urban county.
- Arizona is statewide adoption of the Alliance for Innovation focused on maternal health by all birthing hospitals to ensure the same care is provided in the populous Maricopa County as in the rural Apache County.
- Indiana is to improve obstetric readiness in emergency departments. To do this, Indiana is proposing requiring emergency departments to implement the American College of Obstetricians and Gynecologists’ (ACOG) for obstetric emergencies in non-obstetric settings, including for cardiovascular disease, acute hypertension and eclampsia.
Home Visiting and Care Coordination
Evidence-based home visiting programs supporting pregnant and postpartum people, their newborns, and their families have been to improve newborn outcomes, increase rates of breastfeeding and require less infant emergency medical. Given this, the federal government issued in 2016 to encourage states to design Medicaid benefit packages that provide home visiting services for pregnant people and families with young children. More than half of state Medicaid programs for home visiting services. In their RHTP applications, states are proposing investments in extending care beyond the prenatal and postpartum clinic walls through universal nurse home visiting programs, mobile health clinics and comprehensive postpartum care navigation to ensure safe infant development and maternal recovery.
- Connecticut to expand the state’s Family Bridge nurse home visiting program to support new families. The home visiting model includes perinatal behavioral health screenings, lactation and nutrition support, safe sleep education, and social resources connections.
- Ohio is expanding access to maternal and infant health services through nurse-led home visiting programs in rural and partially rural counties.
- Tennessee expanding the state’s existing integrated model of care coordination, (Community Health Access & Navigation in Tennessee), to 12 rural counties with high rates of sleep-related infant deaths and limited maternity care to provide care coordination and links to community resources.
Maternal Behavioral Health
About one-fifth of the nation’s maternal deaths are to mental health or substance use challenges. As such, states are proposing through RHTP applications to integrate perinatal depression screening into primary care and expand telepsychiatry access lines. Many states are also focused on treating maternal substance use to reduce rates of newborns born with Neonatal Abstinence Syndrome (NAS).
- Georgia is to deploy the telepsychiatry consultation line statewide for maternal health providers to connect with providers specializing in mental health and substance use concerns.
- Virginia to address maternal substance use to reduce the state’s high rate of newborns born with NAS in rural areas, which is 39% higher than the national average. The state proposes the Innovative Maternal Care initiative to treat pregnant and postpartum people experiencing substance use by connecting them to community maternal health hubs and mobile units.
States, providers, health plans, advocates and community-based organizations have significant opportunities through state RHTP programs to improve access to maternal health care services. Together, these cross‑sector partnerships can help stabilize access to maternal care in rural communities, strengthen the workforce and advance more equitable maternal health outcomes long after federal transformation dollars are spent.
For questions on RHT funding for maternal health, please contact or .
March of Dimes 2023 Maternity Care Access by State, available .
Government Accountability Office (GAO). Report to Congressional Committees. Maternal Health: Availability of Hospital-Based Obstetric Care in Rural Areas, available .