
Published On
February 15, 2022
Authors
Service Line Development in Academic Health Systems
Editor’s Note: In a new white paper, summarized below. Manatt Health discusses the important role services lines play in an academic health system’s (AHS’s) strategy, including their critical role in care coordination effectiveness; gating issues for successful service line launch; and the governance, operational and funds flow mechanisms that need to be addressed during development. The paper also covers the financial and operational aspects of implementing an integrated service line in an AHS and presents several real-world case studies analyzing successes, challenges and lessons learned. Click here to download a free copy of the full white paper and here to download our companion webinar, “Creating Successful Integrated Service Lines: A Guide for Academic Medical Centers.”
What Is an Integrated Service Line, and Why Is It Important?
An integrated service line is the coordinated effort of organizing multidisciplinary services—by health condition, organ system, age or gender—across the care continuum to serve a defined patient cohort. Some examples are service lines devoted to cancer, neuroscience, children or women. In other words, an integrated service line is a well-organized model that promotes care coordination among all the specialties required to treat patients in the specified cohort. This structure provides a more patient-centric approach while improving clinical outcomes and efficiencies, facilitating clinical research, and promoting the expansion and integration of high-margin clinical services in an increasingly competitive market. Service lines also facilitate cross-departmental coordination by vesting service line leaders with accountability and responsibility for optimizing clinical services and nonclinical operations.
AHSs have long grappled with the challenge of delivering patient-centric and coordinated care across multiple subspecialists and locations. Service lines can be a highly effective tool in tackling these challenges while keeping the focus on high-quality care and outcomes. In spite of these benefits, academic centers have been slow to realize the potential for multidisciplinary clinical organization. Progressive advances in capability by community-based health systems, however, have raised the stakes. AHSs’ traditional high-margin services have become increasingly price and service competitive as community health systems deliver more advanced tertiary and quaternary services and focus intensely on patient experience. For AHSs to compete successfully, delivering integrated services has become essential.
Gating Issues for Service Line Implementation
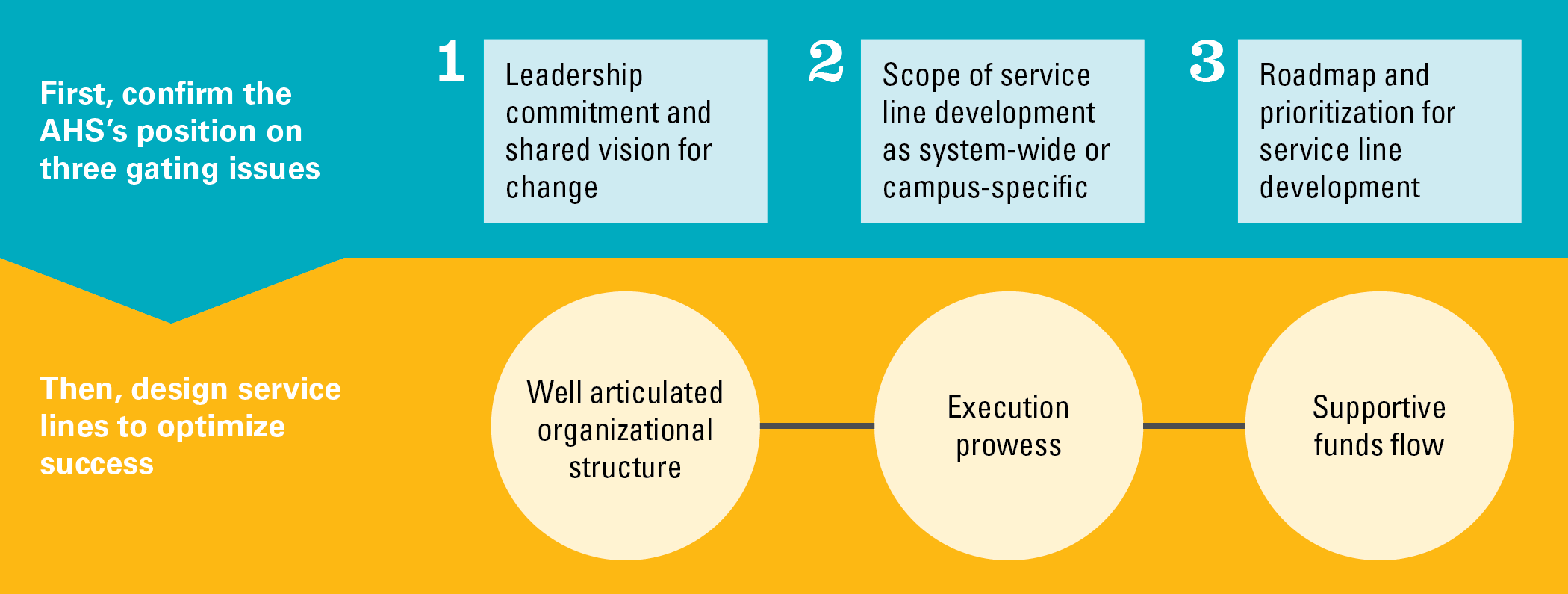
Before implementation of specific service lines can begin, AHSs must address three gating issues:
- Confirming leadership commitment and a shared vision for change at the highest levels
- Defining the scope of service line development efforts as systemwide or campus-specific
- Deciding which integrated service lines to develop and in what order
The first gating issue requires confirming the commitment of leaders at the board, C-suite and dean levels to deliver care through integrated service lines. Implementing this model will require the refinement of existing structures and incentive systems. As with any major organizational change, there will be champions and detractors. Thus, early on and continuously throughout implementation, medical center, health system, practice plan and medical school leaders must clearly articulate how their integrated service line vision supports the shared organizational goals. For many AHSs, these goals include market growth and expanding services to meet patients’ needs. For others, the primary strategic goals may be extending their brand and ensuring consistently high-quality services across their systems.
The second gating issue requires determining whether the AHS’s service lines will be systemwide or campus-specific. While the long-term goal for most AHSs will be to create systemwide service lines, many AHSs have started with their flagship medical center campus and then expanded to the broader health system over time, to manage the pace of change and integration of clinical faculty and community-based physicians.
The third gating issue requires deciding the order in which service lines will be implemented. The criteria for making this decision can include factors such as experience of the faculty and administration, the AHS’s level of expertise and distinction relative to others in the market, and organizational readiness to collaborate across disciplines.
Having prioritized which service lines will be implemented first, leaders should focus on three areas to ensure successful implementation:
- Organizational design, leadership and governance
- Operational execution
- Funds flow
Organizational Design, Leadership and Governance
A well-considered and inclusive design avoids or minimizes tension with medical school departments regarding accountability and authority. Clinical chairs may perceive service line development as a reduction in their authority over key aspects of the clinical practice. However, strong service lines and strong departments are not mutually exclusive—indeed, they have proven to be mutually reinforcing.
We’ve found that successfully implemented AHS service lines feature the following:
- A governance structure with an executive council that will work with and support the service line leaders
- A highly engaged administrative and clinical leadership dyad
- Clarity of roles between service lines and clinical departments
- Accountability for key service line functions that makes clear who is ultimately responsible and makes the final decisions
Operational Execution
Maturation of a fully integrated service line is a multiyear process, and leaders should establish realistic timelines and milestones. During this journey, continued open communication and stakeholder engagement are critical.
Defining the goals and success metrics for the service lines using transparent measures, targets and reporting is essential. The metrics should focus on the AHS’s strategic priorities and may include quality, outcomes, access, patient experience and clinician experience, in addition to financial performance and market position. As the service line team embarks on its implementation journey, leaders should revisit these metrics at regular intervals, at least quarterly.
Setting meaningful goals and organizing service line activities begins with confirming the included patient cohort. Pulling data on historical patients served by the clinical services that will be incorporated into the service line provides a starting point for defining the scope.
Service line leaders should also identify populations the health system is not currently serving. Once a target cohort of current and potential patients has been identified, the collected data should be carefully reviewed and confirmed with the relevant clinical teams to build consensus on the target population. After this initial consultative process, a mechanism must be established for ongoing assessment and reporting of patient needs, as well as service line growth and market potential.
Early in the implementation, the leaders should identify the physicians and staff who will be part of the service line, clearly articulating physician membership or participation criteria, responsibilities, and benefits to ensure accountability.
In the next phase of operational execution, service line leaders need to establish dedicated resources to support execution, such as decision support, network development, business planning, marketing and digital health. The individuals dedicated to the service line for these support services may continue to report to their functional departments, but they should also be accountable to their respective service lines.
Service line development should also include health equity metrics as a foundational component of service line dashboards. As the country reemerges from a pandemic that has disproportionately impacted communities of color, AHSs are shifting out of crisis-response mode and examining opportunities to intentionally promote equity across their clinical, research, and education missions; implement antiracist policies; and bring science to bear in eliminating health disparities in access to and outcomes of care.1
Funds Flow
AHSs are governed by complex and often opaque funds flow arrangements between the hospital/health systems and their schools of medicine/clinical departments. These funds flow arrangements should be viewed as investments that fuel and support joint strategic priorities, including integrated service line development.2 While funds flow arrangements vary widely across organizations, funds often flow through academic departments to compensate faculty effort and provide support for all AHS missions. Seeking to establish integrated service lines as part of the institution’s strategic goals and prioritizing their funding can create tension with department leaders who may view this new direction as a loss of financial control. To address these concerns and align all stakeholders across the enterprise, leaders should follow service line funds flow best practices, which include building an integrated profit and loss (P&L) view of the financial position of each service line and providing adequate investment in the service lines to realize their objectives.
The first step in establishing the funds flow arrangement of an integrated service line is creating a P&L statement that provides an integrated view of the revenues and costs across the health system and the faculty practices that contribute to the service line. Depending on the corporate structure of the entities and their level of integration, service line P&Ls could be operational (i.e., used in day-to-day financial management and reporting) or virtual (i.e., used for reporting and planning purposes). Collaborate with service line leaders to regularly review financial results and, as needed, implement operational interventions.
Successful service line implementation typically includes two types of investments: enterprise base commitments and strategic funds flow investments, which should be aligned to overall funds flow rules and designed collaboratively with department chairs. Enterprise base commitments compensate physicians for their time in providing above-and-beyond services, such as taking on a medical directorship, clinical rounding, call coverage, etc.
Strategic funds flow investments create a “shared risk, shared reward” culture of collaboration across the AHS. They are used to fund faculty recruits, performance incentives, and academic, research and clinical programs. Although strategic funds are time limited, they typically require applicants to submit a plan for how the funded program or initiative will be sustained over the long term via the service line’s regular budget.
Conclusion
Through careful, deliberate organizational design and operational execution, integrated service lines can and should be an important component of an AHS’s organizational development strategy. AHSs and dedicated service line leaders should recognize that this critical work is a multiyear process and that service lines will evolve at different paces depending on an organization’s strategies, needs and leadership capabilities. Service line development is an evolution, not a revolution.
1 Newman, Naomi, et al. “On the Path to Health Justice: How Academic Medicine Can Accelerate an Equitable Health System.” Manatt Health, July 2021, https://www.manatt.com/Manatt/media/Documents/Articles/AMC-Health-Equity-Paper,-Framework-and-Case-Studies-July-2021_c.pdf.
2 Orlowski, J., Enders, T., et al. “Next-Generation Funds Flow Models - Enhancing Academic Health System Alignment.” AAMC – Manatt Health, October 2018, https://store.aamc.org/next-generation-funds-flow-models-enhancing-academic-health-system-alignment-future-of-academic-medicine-series.html.